
In this section, I want to introduce the basics of what is taught in First Responder training as conducted by The Center for Disaster and Extreme Event Preparedness (DEEP). When you look at the DEEP website, you will see that this is actually a very intensive training program.
I am very impressed that there is finally acknowledgement that there is more involved for a fire fighter responding to a house fire than just putting out the fire or to those coming in after a devastating storm than rescue and clean up. These men and women have a primary job to do, yes, but they usually must manage to do that with survivors present. Their jobs will be more doable when they have an insight into the needs of the folks left to live with the aftermath of a crisis. I can’t even imagine how much more complicated a fire fighter’s job is when he/she doesn’t have the skills to manage an hysterical homeowner who could potentially cause more harm because of the level of fear and anxiety they are experiencing.
Medical first aid has three key aims:
Preserve life
Prevent further harm
Promote recovery.
The objectives of Psychological First Aid are very similar and are expressed as:
Restore physical safety
Facilitate psychological function
Empower action
This is succinctly expressed as SAFETY – FUNCTION – ACTION and provides an effective framework upon which to build a training program.
SAFETY
The goals of this aspect of Psychological First Aid are to SAFEGUARD survivors from harm and offer protection by removing them from harm’s way and providing physical safety and security and then to SUSTAIN them by providing basic needs such as shelter, food, water, medical care, clothing, power, light, heat/air conditioning, and sanitation.
FUNCTION
The goals of this piece of Psychological First Aid are to COMFORT those involved by providing soothing human contact, apply stress management techniques, reassure survivors that their reactions are normal and also to CONNECT survivors to family, friends, and social supports.
ACTION
The final goals are to EDUCATE and inform survivors about the disaster – what happened, what will happen, provide guidance about what to do, and identify available resources for support. This reduction of uncertainty is another critical step toward assisting people with recovery. In this phase, it is necessary to EMPOWER survivors to develop realistic plans for disaster recovery and to take first steps toward disaster recovery by helping them identify do-able tasks, and foster self-efficacy and resilience. (Source: Shultz, Cohen, Watson, Flynn, Espinel, Smith. SAFETY, FUNCTION, ACTION Psychological First Aid for Disaster Survivors. Miami FL DEEP Center 2006.)
Here is a great chart from the DEEP website that expresses all these attributes in a clear-cut manner:
Safety – Function – Action
Obviously, one lone First Responder is not expected to provide all these services, especially while performing his/her primary job. However, having First Responders aware of what survivors need and how to connect them with those who can assist further is helpful to everyone involved.
One important detail that is taught to First Responders is that, just like with medical first aid, there is a point where those needing Psychological First Aid need more than first aid. They need more extensive, professional, mental health support. Recognizing when a bandaid is not enough is imperative.
Additionally, when we try to help someone exhibiting signs of Emotional Distress, it is important to realize that our efforts to help may be rebuffed. Despite our best efforts and intentions, sometimes people still become agitated. They may refuse to follow directions, become verbally or physically aggressive, and may otherwise lose control of their normal equilibrium and filters. One bit of counsel I read fit very well in a situation like this: “It is usually not personal. This is their reaction to an UNCOMMON situation, and it has nothing to do with you.” (specific source misplaced)
Something else to keep in mind is that, even though a specific traumatic event is completed, the psychological impact of that event continues for a much longer period. Resolving psychological trauma is not a “take a pill and get over it” proposition. It’s a process. It takes time, as expressed in this chart:
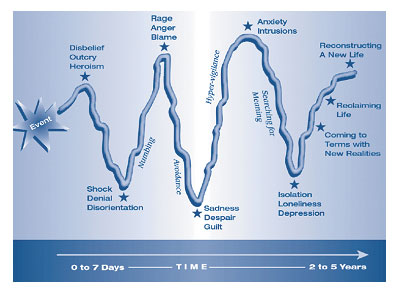
Model of Responses to Trauma Bereavement, CMHS,
1994
Most of us are neither First Responders nor mental health professionals. Nevertheless, we need to develop some level of self-reliance in this area. Like I said in the beginning of this series, the professionals aren’t always immediately available when the need for support arises. Toward that end, the DEEP website includes a free Family Disaster Plan Guidebook that is built around the three principles of SAFETY – FUNCTION – ACTION. I know, there are a lot of preparedness workbooks available on the Internet. This one is definitely worth reviewing.
If you missed the previous episodes of this series, here’s a link back to each:
Disclaimer: Because I am a NOT a professional in this field, my intent with these postings is strictly to show that we need to include Psychological First Aid in our knowledge base just as we do with basic (medical) first aid. I am only reporting what I’ve learned.
Main Source for this segment:
The Center for Disaster and Extreme Event Preparedness
